Is exercise a miracle cure? Or is it just all in my head?
I got sick last week, and I was curious to know what the right volume of training was to optimize my recovery. Luckily, there's a Cochrane review to analyze about this very topic. Let's discuss it.

Top of the morning, sapien. Welcome to Common Sense Medicine, where I try and keep you up to date on the latest and greatest in longevity science. Consistency is a big part of the way that I’ve been living in the past year, and I hate the fact that I’m still in the recovery phase of the illness. It kind of makes me uncomfortable, to be honest, and itching to start doing something. I was able to recover pretty well from this sickness (i.e., < 4 days) which is kind of a record for me, so I’m happy about that at least.
I think part of it was that I was focusing on really getting off the screen instead of laying around and scrolling, which I’m prone to do when I’m confined the house. I focused on getting a lot of science-backed recommendations to recovery, but also the homeopathic ones too including the South Asian endorsed inhaling warm, moist air. There were also a lot of cups of tea consumed, along with a LOT of water.
But, now that it’s almost over, sans a lingering cough which is going away day by day, and I’m ready to jump into the rehab / recovery plan and strengthening to bridge me to the hypertrophy phase beginning in January.
Other items on the differential:
Forward, a care clinic pioneering Medicine 3.0, is shuttering down after raising $100M last year (Business Insider, paywalled)
First instance of reprogrammed stem cells to ‘cure’ Type I diabetes in a 25-year-old (Case Report)

THE WEEKLY DOSE
To exercise or not exercise during sickness?
Last week, we talked about the problem of too much exercise. In today’s newsletter, I wanted to examine a Cochrane systematic reviews of various randomized controlled trials (RCTs) around exercising while sick.
Although I was listening to my body when I decided not to exercise when I was sick, there are times where “listening to my body” became an excuse for not being disciplined. My question was focused on how I can most optimally train while sick, or even optimize recovery so that I can get back to my training goals as fast as possible. Being sick has a nasty habit of derailing even the best of goals. Luckily, I built in a little bit of a buffer in my training plan because I had an inkling that this might happen.
Grande et al had a similar question, namely whether exercise has any effect on the occurrence, severity, or duration of acute respiratory infections.1
What did they do?
Everyone knows that acute respiratory infections (ARI) are the bane of our existence — we usually refer to them as the ‘common cold'. They’re split up into the upper portions (above the glottis / vocal cords) and the lower portions (trachea, bronchioles, and lungs). For this study, they looked at all acute respiratory infections (those which last < 30 days).
The authors noted that usually rest, analgesics (NSAIDs / ibuprofen), antipyretics (i.e., Tylenol), and adequate hydration are indicated for viral ARIs, and antibiotics are indicated for suspected bacterial infection when people have high fever or the infection lasts more than 7-10 days. The authors thought that exercise, a low-cost and readily available intervention, could decrease the occurrence, severity, and duration of ARIs for adults.
They surveyed all RCTs which used exercise in one group compared to those which didn’t do exercise for treatment of ARI (either exercise vs no exercise or exercise vs usual care) and their outcomes were to measure:
The number of ARI episodes / person / year
Proportion of participants who experienced 1 ARI over the study period
Severity of ARI symptoms
Number of symptom days int he follow up period (12 weeks)
Number of symptom days per episode of illness
They found 14 studies which they added to the qualitative synthesis group, and 12 studies which they added to the quantitative synthesis group to see how exercise affects the ARI course.
In order to standardize different scales, they used a standardized mean difference whereas if they had the same scale, they compared using the mean difference. They also used the intention-to-treat analysis for each outcome, which treats people as if they are going to complete the study even if they are going to drop out.
What were the results of this study?
The researchers found that the trials were very heterogeneous. They used the I^2 statistic to measure heterogeneity, which uses the variance between each study to see whether the effect is due to sampling bias (i.e., just because of different populations) or due to an actual treatment effect. In this case, the larger heterogeneity gives us less confidence that exercise is actually the reason for the change, but rather the variation in the different populations.
Second, 12 studies included sedentary participants, and 4 included post-menopausal women. Not really applicable for me, as a younger and more active individual, but I digress. The most common intervention was aerobic exericse (i.e., walking, bicycle, treadmill, or a combination), but also included Qigong (a traditional Chinese healing / exercise technique) and resistance training. Trials differed between protocol for exercise too, with multiple days of exercise per week or consecutively (1 trial was only for 7 days). Studies only compared exercise to no exercise, not exercise to usual care.
Many trials also had issues of attrition bias, or people dropping out of the study. Color me surprised that people don’t want to consistently exercise — have you seen how hard it is in the modern world to get up to do anything? Now, for the money shot — how did the trials do in terms of the primary endpoints?
Not surprisingly, pretty poorly. The number of ARI episodes / person / year, proportion of participants with ≥ 1 ARI in the study period, and number of symptom days per episode of illness were not significantly different between the exercise and non-exercise groups. The things that exercise did make a difference for were the severity of symptoms (as measured by a validated questionnaire) and the number of symptom days in the follow-up period (12 weeks), where the exercise group had 2 fewer symptom days. Again, these findings had a limited level of evidence score due to the heterogeneity of the mode of exercise, the study design, and lack of blinding with result to the outcomes. Even with a robust sensitivity analysis, it was hard to find any significance between exercise and the primary outcomes which they were shooting for.
My thoughts about this review
One thing off the bat which I noticed was that most of the trials were looking at sedentary people, with a skew towards women-only trials. Even though the study results are hardly generalizable, maybe these results can be partly relevant to a patient population which is struggling with obesity. It shows that symptom severity can decline even if you’re moderately active, such as 10 minutes on the bike, or 20 minutes walking. The authors do say that they only included moderate exercise, so it’s hard to say whether they would have had a different conclusion had they separated trials which only included ‘high intensity’ exercise specified by a cutoff. There is another paper by Lee et al which did consider this and showed more promising results, but that is an analysis which I’ll save for another day.
My second gripe with this study was that the types of exercise that were included were so different, partly because there isn’t much great data about specific modalities of exercise on sickness occurrence or severity. I mean, Chinese healing could have a way different intensity than a Zone 2 bike workout, but grouping them makes it hard to identify specific sub-group effects. Out of these, the vast majority used moderate aerobic exercise, so I’m hoping that the effects on severity and symptom days on follow-up might say something about this particular mode of exercise rather than others.
Third, the limitation which the authors already noted was that the trials weren’t blinded — although, to be fair, it’s not like you’re giving them a pill. Participants will know who is exercising and who is not.
Moving onto the actually statistically significant portions of the study, let’s look at the severity and the symptom days in the follow-up. Okay, so the review shows a pretty modest effect size for the the two primary outcomes, as expected. Only 2 trials reported the severity of symptoms — Barrett 2012 and Barrett 2018. Let’s look at these trials in further detail to tease out the protocol we’d want to use when thinking about our (read = my) training protocol for ‘preventing sickness’.
Figure 1 (from Grande et al)

In both trials, Barrett et al (2012 and 2018) was trying to figure out whether meditation vs. exercise vs. nothing would reduce the severity and the mean days of illness per person. There were two trials — MEPARI-1 and MEPARI-2. They didn’t take my suggestion to title it MEPARI-2-FAST-2-FURIOUS.
I guess the Cochrane review wholesale discarded the meditation group, but Barrett et al showed in MEPARI-1 that the meditation group actually did better than the exercise group. But, this conclusion is muddied by MEPARI-2, which may cast some doubt on the conclusion that meditation truly had a better outcome than exercise. I’m taking this as a wash, saying that both could possibly be effective, from a psychologic and physical standpoint.
Figure 2 (from Barrett 2018)

Conclusion and takeaways
Okay, this is getting long - what’s the upshot? Basically, I think that the benefits that we’re seeing here is that moderate exercise like biking, stretching, or walking does reduce the severity of ARI symptoms. I think in an n = 1 case, during my sickness last week, I thought that I got over this cold pretty quickly — maybe 2 days faster than I normally do. This timeline tracks with the results of this study, which is encouraging. I think I’m not really changing my protocol of exercise based on this study, although it would be helpful to add in meditation based on Barrett et al.
I talked about breathing and prana as a treatment for pulmonary diseases, and I’m yet to try and include that in my training. But maybe, I’ll do another review of what the evidence is focused on and how to incorporate that within a bigger systematized framework going forward. Until then, I’m going to continue to end out the year on a 2x week biking / aerobic fitness cycle and the strength training which I have already protocoled in prior issues (4x week).
It’s hard to conclude anything from this pretty inconclusive study other than — do some biking and do some meditation as well on a regular basis. Your body will thank you when you get infected with a cold, as mine did.

FIGURE OF THE WEEK
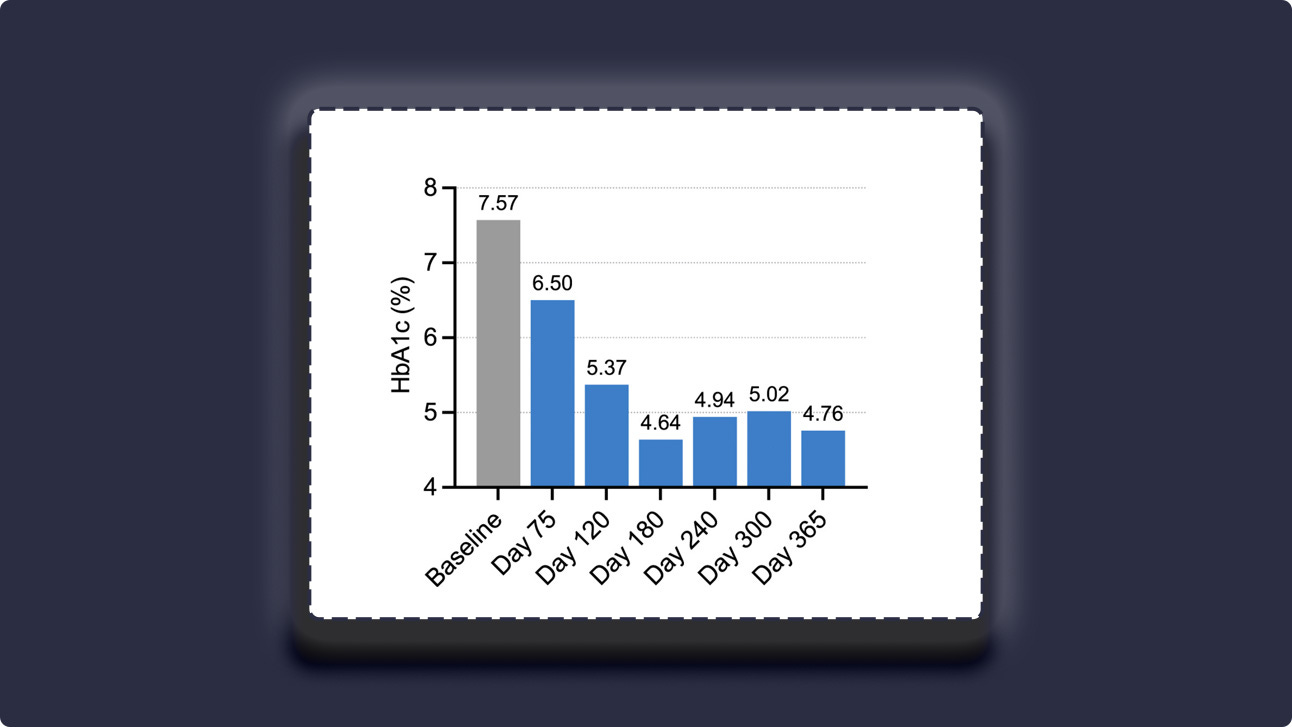
The upshot: After being transplanted with her own stem cells which were pre-programmed to create insulin endogenously, a 25-year-old female with a history of Type I Diabetes decreased her HbA1c from 7.0% (squarely in diabetic range) to a cool 4.76%.
More information: The patient was injected with chemically induced pluripotent stem cells and was on an immunosuppressive regimen for the whole experiment, however, this shows the potential of stem cell therapy reprogramming to revolutionize how we treat diabetes. Although there is a chance of graft-related malignancy, with the tendency for stem cells to revert back to their previous forms, I’m hopeful that we can see some of these gene therapies come to clinic at some point in the future. The stability of the response post-transplant for a year gives me hope that this is not just a fleeting therapy2

REMEMBER, IT’S JUST COMMON SENSE.
Thanks so much for reading! Let me know what you thought by replying to this email.
See you next week,
Shree (@shree_nadkarni)
The information provided here is not medical advice. This does not constitute a doctor patient relationship and this content is intended for entertainment, informational, and educational purposes only. Always consult with a doctor before starting new supplementation protocols.
Grande AJ, Keogh J, Silva V, Scott AM. Exercise versus no exercise for the occurrence, severity, and duration of acute respiratory infections. The Cochrane Database of Systematic Reviews. 2020;2020(4):CD010596. doi:10.1002/14651858.CD010596.pub3
Wang S, Du Y, Zhang B, et al. Transplantation of chemically induced pluripotent stem-cell-derived islets under abdominal anterior rectus sheath in a type 1 diabetes patient. Cell. 2024;187(22):6152-6164.e18. doi:10.1016/j.cell.2024.09.004